Most people have never heard of IgA deficiency - and that’s okay, because for 90% of those who have it, they never know they have it at all. But for the other 5 to 10%, this quiet immune flaw can turn a simple blood transfusion into a life-threatening event. IgA deficiency isn’t just a lab result. It’s a real, documented condition that affects about 1 in every 500 people in the U.S. and Europe. And if you’re one of them - or someone caring for someone who is - knowing what to watch for and how to protect yourself can make all the difference.
What Exactly Is IgA Deficiency?
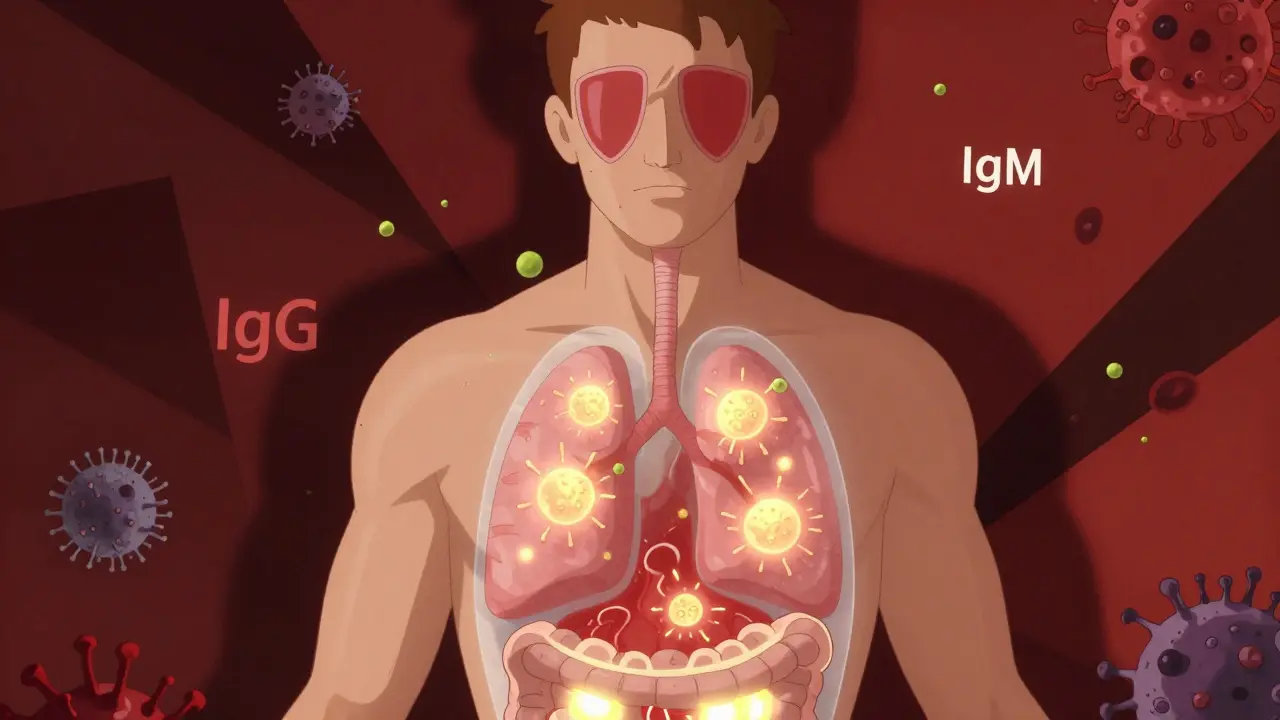
Immunoglobulin A, or IgA, is the antibody your body uses to guard the surfaces where you meet the outside world: your nose, throat, lungs, gut, and eyes. It’s not in your bloodstream like IgG or IgM. It’s on the front lines. When you breathe in pollen, swallow food, or get a cold virus, IgA is the first immune response trying to stop it before it gets inside.
Selective IgA deficiency means your body makes little to no IgA - less than 7 mg/dL in the blood. Everything else, like IgG and IgM, works fine. That’s why it’s called "selective." Your immune system isn’t broken overall. It’s just missing one key soldier.
This isn’t something you catch. It’s genetic. If a close family member has it, your chances of having it go up 50 times. It’s not caused by drugs or infections. It’s just how your immune system was built.
Do You Even Know You Have It?
Most people don’t. They live their whole lives without symptoms. No frequent infections. No allergies. No digestive problems. They get blood tests for other reasons - maybe before surgery or during a routine checkup - and find out they’re IgA deficient by accident.
But for those who do have symptoms, it’s not minor. About half of symptomatic people get repeated infections in their sinuses, ears, and lungs. Think ear infections in kids, sinus infections that won’t quit, bronchitis that turns into pneumonia. These aren’t one-off colds. These are the kind that come back every few months, even with antibiotics.
Then there’s the gut. Around 1 in 5 people with IgA deficiency have chronic diarrhea, often from giardia - a parasite that shouldn’t stick around in healthy people. About 1 in 10 develop celiac disease. That’s not just gluten intolerance. It’s an autoimmune reaction where your body attacks your own intestines. And if you have IgA deficiency, standard celiac tests (which rely on IgA antibodies) can give false negatives. You need a different test - IgG-based - to catch it.
Allergies are also common. About 1 in 4 people with IgA deficiency have eczema, asthma, hay fever, or allergic conjunctivitis. It’s not that IgA deficiency causes allergies. It’s that the same immune imbalance that stops IgA production also makes your body overreact to harmless things like dust or pollen.
The Hidden Danger: Blood Transfusions
This is where things get dangerous - and why this condition isn’t just a footnote in medical textbooks.
When your body doesn’t make IgA, your immune system sometimes decides it’s a foreign invader. So it makes antibodies against it - anti-IgA antibodies. About 1 in 3 people with IgA deficiency develop these. And if they ever get a blood transfusion with normal IgA in it? Their immune system goes into overdrive.
That’s not a mild reaction. That’s anaphylaxis. Within minutes, your blood pressure can crash. Your airways can swell shut. Your heart can struggle to keep up. About 15% of these reactions are life-threatening. And in 10% of cases, they’re fatal.
And here’s the scary part: it can happen on the very first transfusion. You don’t need to have had blood before. If you’re IgA deficient and have anti-IgA antibodies, the first unit of blood you get can kill you.
That’s why doctors don’t just say "be careful." They require proof - and preparation.
What Happens If You Need a Transfusion?
If you’re diagnosed with IgA deficiency and need blood - whether for surgery, trauma, or anemia - you can’t just get any blood bag off the shelf.
You need either:
- IgA-depleted blood products - processed to remove nearly all IgA (less than 0.02 mg/mL), or
- Washed red blood cells - rinsed multiple times to strip away plasma proteins, including IgA.
Both options cost about three times more than regular blood. They’re not kept on the shelf. You need to order them in advance - often 48 to 72 hours before surgery. That’s why planning ahead is non-negotiable.
Before any transfusion, you should also be tested for anti-IgA antibodies. The test - called an ELISA - is 95% accurate. But 5 to 10% of the time, it misses them. So even if your test is negative, if you’re IgA deficient, your doctors should still assume you’re at risk and use special blood.
What Should You Do If You Have IgA Deficiency?
You’re not alone. But you’re also not invisible. Here’s what you need to do right now:
- Get confirmed diagnosis - If you’ve had repeated infections, celiac disease, or unexplained allergies, ask your doctor for a serum immunoglobulin test. Make sure they check IgA, IgG, and IgM levels.
- Carry medical alert identification - Wear a bracelet or carry a card that says: "Selective IgA Deficiency - Requires IgA-Depleted or Washed Blood Products." Emergency responders don’t know your history. They need to see it in bold.
- Inform every doctor - Dentists, surgeons, OB-GYNs, even your primary care provider. Every time you’re scheduled for a procedure where blood loss is possible, remind them. Put it in your electronic medical record.
- Know your transfusion options - Ask your hospital’s blood bank if they stock IgA-depleted products. If not, find a center that does. Don’t wait until you’re in the ER.
- Get screened for related conditions - Annual celiac testing (IgG-based), biannual lung function tests, and regular checkups for autoimmune diseases are part of long-term care.
Patients who do these things reduce their risk of a transfusion reaction by over 90%. The Immune Deficiency Foundation reports that 65% of IgA-deficient people feel anxious about emergency care - and 42% have been treated by doctors who didn’t know what to do. You can change that for yourself - and for others.
What About Treatment?
There’s no cure. You can’t take a pill to make your body produce IgA. But you can manage the consequences.
For infections: antibiotics when needed, and sometimes preventive antibiotics if you’re getting sick too often.
For celiac: strict gluten-free diet - no exceptions.
For allergies: standard treatments like antihistamines or inhalers.
For transfusions: the special blood products are the only proven way to stay safe.
There’s new hope on the horizon. Researchers are testing recombinant human IgA - lab-made IgA that could be given as an infusion. So far, only 12 people worldwide have received it in trials. It’s not available yet. But it’s a sign that science is catching up.
What’s the Long-Term Outlook?
Most people with IgA deficiency live normal, full lives. A 20-year study found that 95% have a normal life expectancy. The key is avoiding complications - especially those triggered by transfusions or undiagnosed autoimmune diseases.
The 5% who develop severe problems - like bronchiectasis (permanent lung damage from repeated infections) or aggressive autoimmune disorders - do face reduced life expectancy. But even then, early detection and careful management can help.
This isn’t a death sentence. It’s a condition that demands awareness. And awareness is something you can control.
Can IgA deficiency be cured?
No, there is no cure for selective IgA deficiency. The body doesn’t start producing IgA on its own. Treatment focuses on managing symptoms and preventing complications - especially avoiding transfusion reactions by using IgA-depleted or washed blood products.
Can I donate blood if I have IgA deficiency?
No. People with IgA deficiency should not donate blood. Their blood contains anti-IgA antibodies, which could trigger severe reactions in recipients who are also IgA deficient. Blood banks screen for this and will defer donors with known IgA deficiency.
Is IgA deficiency the same as common variable immunodeficiency (CVID)?
No. IgA deficiency is isolated - only IgA is low. CVID involves low levels of multiple immunoglobulins (IgG, IgA, and sometimes IgM) and causes more severe, widespread infections. People with CVID often need regular IVIG infusions. IgA deficiency is much more common and usually less severe.
Why do some people with IgA deficiency have no symptoms?
The immune system has backups. Other antibodies like IgG and IgM can compensate in many cases. Also, IgA’s main role is on mucosal surfaces - if you’re not exposed to frequent pathogens or have a strong overall immune response, you might never notice the lack of IgA.
Should I get tested for IgA deficiency if a family member has it?
Yes. If a close relative has IgA deficiency, your risk is 50 times higher. Even if you feel fine, getting tested can prevent dangerous situations - especially if you ever need surgery or a blood transfusion. The test is simple: a blood draw to measure IgA, IgG, and IgM levels.
Can children outgrow IgA deficiency?
In rare cases, yes - especially in young children. Some kids with low IgA levels at age 2 or 3 may normalize by age 5 or 6. But in adults, IgA deficiency is almost always permanent. Testing should be repeated if diagnosed in childhood to confirm persistence.
What’s Next?
If you’ve just been diagnosed, take a breath. You’re not broken. You’re just different - and now you know how to protect yourself.
Start by talking to your doctor about a personalized care plan. Get your medical alert ID. Make sure your family knows what to do in an emergency. And don’t let fear silence you. The more people who speak up about IgA deficiency, the safer it becomes for everyone with it.
This isn’t a condition you can ignore. But it’s one you can manage - if you know the rules. And now, you do.




Sahil jassy
December 18, 2025 AT 13:01Kathryn Featherstone
December 18, 2025 AT 18:35mary lizardo
December 18, 2025 AT 22:21shivam seo
December 19, 2025 AT 19:49Andrew Kelly
December 21, 2025 AT 10:11Anna Sedervay
December 22, 2025 AT 13:38Matt Davies
December 22, 2025 AT 13:59Mike Rengifo
December 23, 2025 AT 02:04Ashley Bliss
December 24, 2025 AT 02:55Dev Sawner
December 25, 2025 AT 18:57Moses Odumbe
December 27, 2025 AT 06:21Meenakshi Jaiswal
December 27, 2025 AT 23:17bhushan telavane
December 28, 2025 AT 21:34pascal pantel
December 29, 2025 AT 03:37